A conversation with social designer Joes Janmaat (Studio Sociaal Centraal) and nephrologist Karin Gerritsen (UMC Utrecht) about the Watercare project, social design in healthcare, and why caring for water is not radical, but simply the right thing to do.
This is the second article in the series Imagining Circular Futures for Hospitals, following on from the exploration phase described in our first article. Here, we zoom in on one of the concrete initiatives that grew out of that exploration: the Watercare project at UMC Utrecht’s dialysis department.
What is Watercare?
Watercare (Waterzorg) is a concept originally coined by KWR Water Research Institute as part of their GRROW programme, which develops new language for our changing relationship with water. In this project, the term has been adopted to give a name — and a face — to the work happening at UMC Utrecht’s dialysis department. The core idea is straightforward: if hospitals care for people, it is only logical that they also care for water. Watercare is not just a technical project; it is a shift in perspective, from treating water as an invisible, cheap commodity to recognising it as something worth caring for.
Waterzorg: A word that fits
When asked to explain Watercare to someone encountering the concept for the first time, Joes Janmaat and Karin Gerritsen approach it from different but complementary angles.
Joes Janmaat: Watercare is a concept, a word that was coined by KWR Water Research Institute, and it fits perfectly with the work that Karin and her colleagues are already doing. It gives that work a face. Watercare means that it is logical — not radical — for us as people to care for water in order to care for people. That if you work in healthcare, in a hospital, on a dialysis ward, caring for water is simply part of caring for patients.
Karin Gerritsen: I come at it from a very practical angle. We use an enormous amount of water; the equivalent of an Olympic swimming pool per year, just on the dialysis ward. And we hardly ever think about it, because water is so cheap and always available. But that is changing. Even in countries like the Netherlands, water scarcity is becoming a real issue, which means we will need to think much more carefully about the use of water. The water that leaves our department also contains medication residues that can contribute to antibiotic resistance, hormonal disruption in aquatic life, and eutrophication (the excessive enrichment of water with nutrients, which causes harmful algal growth and oxygen depletion). If we can clean it at the source, we prevent problems further down the line. Thus for me, Watercare means using water responsibly.
“We use the equivalent of an Olympic swimming pool of water per year, just on the dialysis ward. And we hardly ever think about it.” — Karin Gerritsen
Why dialysis?
Dialysis is one of the most water-intensive treatments in a hospital, which makes it both the most urgent and the most illustrative starting point for circular water management. Karin explains how the process works, and where the water waste occurs.
Karin: During haemodialysis, the patient’s blood is filtered through a membrane. On the other side runs a dialysis fluid — dialysate — that draws waste substances out of the blood. Producing that dialysate requires large volumes of ultrapure water. Historically, two thirds of the water used was needed to make one third of usable dialysate — and that two thirds went straight down the drain, even though it was still remarkably clean. Today, we have already brought that ratio down to roughly fifty-fifty, which means we are wasting significantly less water than before.
And there is important news: a greywater reuse system has been included in the programme of requirements for the major redevelopment of UMC Utrecht’s dialysis department, as part of the major redevelopment of UMC Utrecht. That means the clean waste water that currently disappears into the sewage system will be captured and reused, for example to flush toilets. That is a real milestone, because it means circular water management is now built into the future infrastructure of the hospital.
Joes: When we started working together, it was not yet clear whether any of this would even be feasible. But things have moved incredibly fast. The fact that water reuse is now part of the plans for the new building shows that this is no longer an experiment. It is becoming the standard.
The role of social design
The Watercare project is a collaboration between clinical research and social design; two disciplines that do not often meet. Joes describes how the design work complements Karin’s research by making the story accessible and engaging for a wider audience.
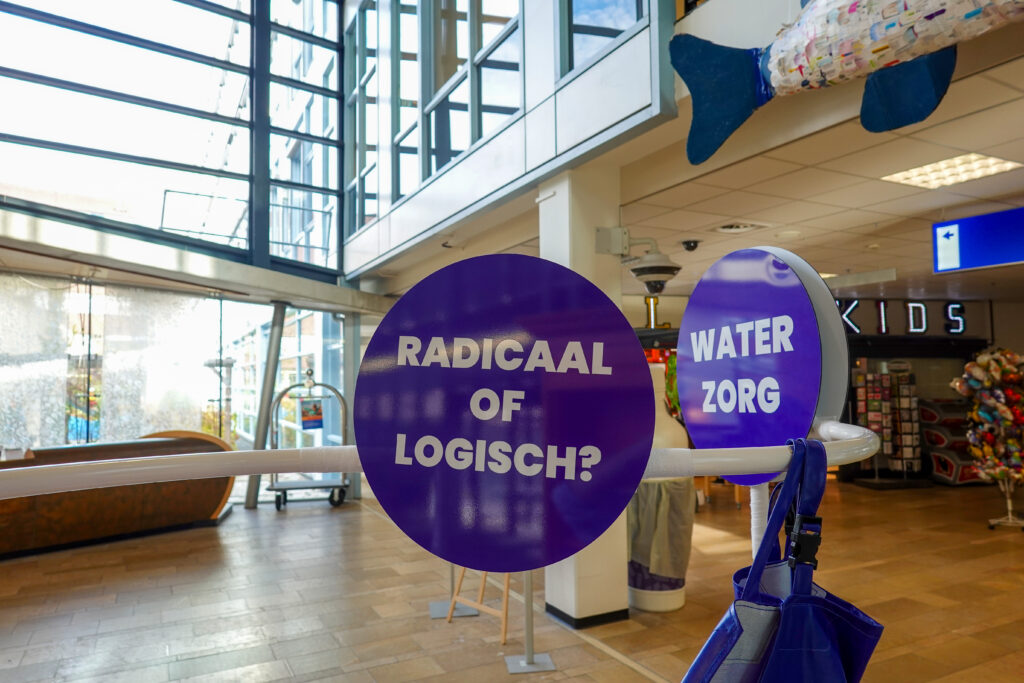
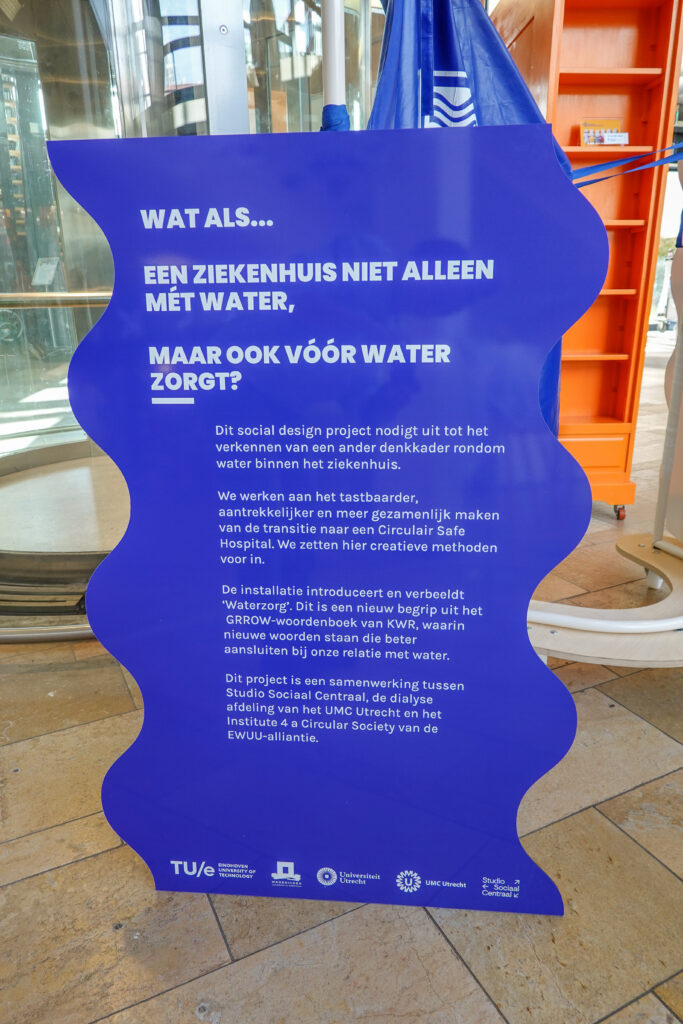
Joes: The design side of what Karin and I do together is about making the work more creative, more collaborative, and more visible. Karin’s research is essential — the measurements, the interventions, the technical innovations. What we add as designers is a way to take people along in the story. We have experimented with different approaches: a guided reflection exercise that invites people to connect with water, an installation that was part of the Circular Art Expo at UMC Utrecht, and visual materials that make the facts tangible. Think of how much water is used, where it goes, and what the future could look like.
“What we add as designers is a way to take people along in the story.” — Joes Janmaat
We introduced the idea of ‘watercarers’ (waterzorgers): people within the hospital who embody the message that caring for water is logical. And we created visuals that juxtapose the current situation with a future perspective: ‘Remember when clean, reusable water disappeared down the drain? Remember when medication residues polluted rivers and ditches?’ That reframing — from how things are now to how they could be — is what social design can do.
Small changes, big savings: what the measurements show
Beyond the design work, the project is grounded in concrete measurements and practical interventions. Karin describes how surprisingly simple changes have already made a significant difference, and why publishing those findings matters for other hospitals.
Karin: We have carried out detailed measurements and discovered that water savings can be achieved through surprisingly simple interventions. For example, we found that machines were running continuously, using 500 millilitres of ultrapure water per minute while waiting for a patient to be connected, sometimes for half an hour or more. Thanks to Guus Crooijmans, dialysis nurse and member of the green team, new protocols were introduced so that dialysis nurses now switch the water flow off after the priming period and turn it back on when the session actually starts. A small behavioural change, but a significant reduction in valuable resources used.
We also found that the water purification system continued running at more than 1 L per minute when no hemodialysis sessions were scheduled, and that its purification performance far exceeded what was required. The ultrapure water consistently contained electrolyte levels so low they could not be detected. So we have been able to increase the concentration factor of the reject water, meaning less water is wasted. And the remaining waste water stream is still clean enough to be reused for example for flushing toilets, cleaning windows, and watering plants.
“Sometimes the biggest impact comes from the simplest changes, like switching off a machine that was running for nothing.” — Karin Gerritsen
We plan to publish these findings this year. It may not sound like groundbreaking research, but it is an eye-opener for other centres. If you simply start measuring, you may find that there is much more you can save than you thought.
There is also an exciting new development: the division has recently approved the purchase of a Dialysis Unit Monitoring System that provides real-time insight into water and energy consumption. Until now, flow and energy meters had to be hired and installed temporarily. A cumbersome process. The new system will make it possible to optimise and reduce consumption on an ongoing basis, and to report findings to staff, helping to build wider awareness across the department.
At the same time, we are working on innovations such as a water- and energy-saving alternative to the current water purification system, as well as regeneration of spent dialysate to enhance circularity.
From green nephrology to the ICU: growing interest across borders and departments
The impact of the project is already reaching well beyond the dialysis ward. Karin has presented the work at international conferences, and interest is coming from unexpected corners — from other hospital departments, from European research projects, and from countries where water scarcity makes circular approaches not just logical but essential.
Karin: Internationally, there is considerable interest. I have already presented our measurements and interventions at conferences and we have given webinars on optimising water use. Nephrologists from Morocco, Tunisia, and Australia have reached out to us. These are regions where water scarcity is a daily reality, the urgency is even greater. In some places, water for dialysis has sometimes to be delivered by lorry.
Within UMC Utrecht, the intensive care unit has also expressed interest. They use substantial volumes of medication and antibiotics, so the wastewater challenges are comparable. And there is a large EU sustainability project, led from the Ireland, that wants to explore whether our approach can be applied more broadly.
Joes: That is exactly what I hope the design side contributes to. By making this work visible and tangible, it becomes easier for others to see that it is logical — and to feel motivated to act. The Watercare concept can travel. The creators of the term itself, at KWR, are interested in how the work has been made experiential and whether this approach could be used elsewhere.
A permanent home, a pop-up installation, and the quest to regenerate dialysate
The project is entering a new phase: from experimentation to a permanent presence in the hospital, and from local impact to broader ambitions. Both Joes and Karin look ahead to what is coming.
Joes: Watercare is getting a permanent place in the ‘Care of Tomorrow’ exhibition at UMC Utrecht’s main entrance. That is significant. Water was not originally part of that exhibition at all. We are also developing a pop-up version of the installation that can be taken to conferences and events, so that Karin and her colleagues can bring Watercare wherever they go.
“We have already come a long way. Simple interventions, awareness, measurement — these things add up.” — Karin Gerritsen
Karin: On the research side, we are looking into the ultimate step: full regeneration of dialysate. That would mean reusing the dialysis fluid itself during a patient’s session, rather than discarding it. We are conducting a feasibility study to see whether existing technology can make this work. We are also exploring biomimetic membranes — membranes that use the body’s own water transport channels, called aquaporins — developed by a company in Denmark. If successful, this could dramatically reduce both water and energy use. But that is genuinely complex, and we are still in the research phase.
What I do want to emphasise is that we have already come a long way. Simple interventions, awareness, measurement — these things add up. And the fact that there is approval for the greywater system for the new department shows that this is being taken seriously at every level.
Research and design as partners in change
Towards the end of the conversation, the question arises naturally: how do these two very different approaches — clinical research and social design — actually reinforce each other?
Joes: Karin and her colleagues work incredibly hard, and the research is heading in the right direction regardless. But I hope that the creative side acts as a lever — a way to make more people feel that this is logical. That it is not just Karin who has to push for change, but that it becomes a shared conviction. If people see the installation, hear the story, feel the scale of water use, it shifts something. And that makes it easier for the practical changes to happen.
Karin: I agree. It does help. Getting people on board for something that sounds simple can still be surprisingly difficult in a hospital setting. The design work creates shared language, a sense of purpose. It makes what we are doing more visible — and visibility helps drive change.
From radical to logical
What stands out from this conversation is how naturally research and imagination come together when the goal is clear. Watercare did not start with a grand plan; it started with measuring, with asking questions, with making things visible. A nephrologist who noticed how much water was being wasted. A social designer who saw the potential to turn that insight into something people could feel and talk about. And a shared conviction that caring for water in a place that cares for people is not radical at all. It is simply logical.
The Watercare installation will soon have a permanent home at UMC Utrecht. The research continues. And the idea — that everyone can be a watercarer — is already travelling further than anyone expected.
About the interviewees

Joes Janmaat is a social designer at Studio Sociaal Centraal, working on projects that use design and imagination to address complex societal challenges. For the Watercare project, Joes develops installations, experiments, and visual materials that make the case for circular water use in hospitals tangible and accessible.
Karin Gerritsen is a nephrologist and associate professor at UMC Utrecht, specialised in kidney replacement therapy dialysis. Alongside her clinical work, she leads research into water reduction, waste water reuse, and circular innovations on the dialysis department. She has presented this work at international conferences and contributes to the EWUU Alliance’s work on circular healthcare.
.
This article is part of the series Imagining Circular Futures for Hospitals, which follows how creativity, research, and social design can accelerate the transition towards circular healthcare. Read the first article in the series to learn more about the exploration phase and the broader context of this work. Learn more about Watercare, including the guided reflection exercise.
The Waterzorg installation at UMC Utrecht
Photos by Studio Sociaal Centraal